Article Text

Abstract
Background and aims Research on the importance of the Emergency Medical Dispatch Centre (EMDC) role in reducing the time delays for patients with acute ischaemic stroke (AIS) is limited. This study aimed to analyse how Norwegian EMDCs’ accurate suspicions can impact the clinical care times in this patient group.
Methods We collected clinical care time metrics and acute reperfusion treatment data from the Norwegian Stroke Registry on patients with AIS in Western Norway who were evaluated by the EMDC and had an ambulance dispatched in 2021. In case a stroke was suspected by the EMDC, the dispatcher communicated their diagnosis suspicions to the ambulance personnel. Outcomes of interest were reperfusion treatment for AIS, prehospital and in-hospital time-to-treatment delays, and patient outcomes.
Results Of the 1106 patients with AIS in our region, 771 (70 %) fulfilled the inclusion criteria. The EMDC suspected a stroke in 481 cases (62 %). Patients with suspected stroke experienced lower ambulance on-scene times (11 min vs 15 min; p=0.001), Emergency Medical Service prehospital times (40 min vs 49 min; p=0.021) and door-to-needle times (23 min vs 31 min; p=0.023). The EMDC stroke suspicion was associated with increased thrombolysis rates (OR 2.42 (95% CI 1.72 to 3.40)) after adjusting for age, sex, risk factors and functional status prior to the stroke event. The door-to-groin puncture times were lower for patients with a stroke suspicion who received endovascular treatment (65 min vs 85 min; p=0.004). No differences in the National Institutes of Health Stroke Scale score at the initial hospital arrival (4 vs 4; p=0.42) or in 90-day functional independence outcomes (rate of modified Rankin Scale score 0–2; 240 (61%) vs 160 (66%); p=0.24) were observed.
Conclusions Accurate EMDC recognition of stroke suspicion alerts to ambulances were associated with a reduction in time until treatment and increased intravenous thrombolysis rates. A significant proportion of patients who had a stroke were not identified by the dispatcher. Improving dispatcher stroke assessment training, tools and knowledge may reduce time delays, thus improving patient outcomes.
- death
- stroke
- triage
- emergency care systems
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prehospital on-scene identification of acute ischaemic strokes is associated with reduced Emergency Medical Service (EMS) time delays, higher rate of reperfusion treatments and lower mortality risks.
Some studies suggest that the dispatcher recognition of stroke is also associated with reduced EMS time delays and higher reperfusion treatment rates.
However, limited studies have analysed the associations between dispatcher recognition of stroke on the speed of all aspects of the acute stroke chain, from the dispatch contact to administration of intravenous thrombolysis and endovascular treatment.
WHAT THIS STUDY ADDS
In this study, using Norwegian stroke registry cases from one health region in 2021, the dispatcher recognition of stroke was associated with increased reperfusion treatment rates and a reduction in both prehospital and in-hospital time delays.
However, a significant proportion of patients who had acute ischaemic stroke are not identified by the dispatcher, and we found that a lack of recognition of stroke was associated with treatment delays and lower reperfusion treatment rates.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Dispatcher identification of stroke is associated with reperfusion treatment rates through reduction of prehospital and in-hospital time delays.
Methods to improve dispatcher training, recognition and auditing are needed.
Background
Stroke is one of the most common cardiovascular diseases necessitating swift medical attention and the prompt administration of intravenous thrombolysis (IVT) and endovascular treatments (EVTs) to reduce morbidity and mortality.1 2 The outcomes following acute ischaemic stroke (AIS) are highly correlated with onset-to-treatment times.3–5 A significant proportion of patients fail to reach the hospital in the therapeutic time window for reperfusion despite the availability of effective treatments.6 The bystander misidentification of strokes and diagnostic delays by Emergency Medical Service (EMS) are two well-documented factors.7 8 There is increasing evidence indicating inadequacies in the whole system’s organisation and effective prehospital stroke management, emphasising the need for more research on improving the learning effectiveness across the acute stroke chain.
The Emergency Medical Dispatch Centre (EMDC) regularly serves as the initial contact point for patients with AIS seeking medical attention. One study in Norway reported that around two-thirds of patients who had stroke initially contact the EMDC.9 The emergency levels and problem codes are determined based on the EMDC operator’s assessment of the patient’s symptoms and medical severity during the emergency call. Prompt recognition and accurate identification of symptoms compatible with stroke by the EMDC operators are essential for ensuring the timely and correct dispatch of EMS resources for effective prehospital management.10 Most EMDCs use the Medical Priority Dispatch System (MPDS) to assess the severity of medical and trauma cases. The MPDS scale, developed during the 1980s, can help improve the dispatch triage of critically ill patients.11 However, the MPDS is variable in its performance, accuracy and external generalisability for optimal AIS identification and treatment.12
Research on the significance of early EMS arrival for on-scene stroke assessments has demonstrated its impact on minimising time delays and led to improved outcomes.13 Limited studies, however, have investigated the downstream and longer-term effects of dispatch accuracy and performance.
The objective of the study was to determine if there is an association between an accurate suspicion of stroke by Norwegian EMDC dispatchers and clinical care times in patients with AIS.
Methods
Study population and design
This registry-based observational study from the Norwegian Stroke Registry (NSR) enrolled patients diagnosed with AIS (International Classification of Diseases, version 10 (ICD-10) code I63) who were admitted directly to hospitals after contacting the EMDC in Western Norway from 10 January to 31 December 2021. The NSR is a mandatory reporting system in which all Norwegian hospitals are legally required to report information on patients with AIS for quality measurement, improvement and reporting purposes.14 The study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) standards.
Setting
The EMS in Norway are organised under local hospital trusts, which in turn are managed by regional health authority trust and financed by the national government. The EMS in Norway primarily consists of the Emergency Medical Dispatch Centre (EMDC) and ambulance services. The EMS cooperate with the hospital’s ED and municipality-based emergency rooms (ERs). The ERs in Norway manage low-risk patients who do not need hospital admission or specialist consult.
The EMDC is a medical dispatch centre for coordinating and managing ambulance responses to medical incidents. Nurses and ambulance coordinators work in EMDC teams of two and manage all aspects of a call, from the initial interview phase to dispatching and on-scene arrival. The operators undergo regular courses in emergency medicine. The EMDC uses a selective medical dispatch system to dispatch ambulances, air ambulances and first responders. Dispatchers collect information from callers, including the type of emergency, location of incident, medical state of the patient and provide first aid caller guidance. They assign an emergency level and a diagnostic suspicion at the time of the initial call using the Medical Priority Dispatch System (MPDS) scale.15 The dispatch emergency level is based on the dispatcher’s understanding and suspicions during initial contact with callers about their medical condition. The stroke suspicion assessment routinely includes face-arm-speech-time (FAST), visual loss, coordination disabilities and headache symptom screening, which was assessed by a combination of open-ended and categorical (yes/no) questions by the EMDC operator on phone. If the dispatcher has a suspicion of a stroke, this is communicated to the ambulance personnel.
In the Norwegian EMDCs, the three levels of emergency dispatch are acute, urgent and routine with their own colour codes (red, yellow and green). According to Norwegian quality indicators, 90% of emergency dispatches with acute (colour code red) priority need to be on-scene within 12 min in urban and 25 min in non-urban areas after the initial EMDC contact.16 For urgent and routine dispatches, there are no response time requirements. Stroke, myocardial infarction, cardiac arrest, trauma and sepsis are regarded as critical medical conditions that require an ambulance dispatch at the highest emergency level. For all these conditions, hospital prenotification by ambulance is mandatory.
The catchment area for this study includes patients from Norwegian hospital trusts in the majority of Vestland and Rogaland counties, serving a population of 920 000 and spanning an area of 32 000 km². The four EMDCs in the study region deploy a fleet of 75 ambulances, three physician-staffed air ambulances and two physician-staffed search and rescue helicopters. All ambulances are equivalent to advanced life‐saving units with regard to equipment, type of assignments and competence level of clinicians. In our health region with four EMDCs, the centre with the lowest call volume responds to 12 000 and the busiest to 61 000 emergency calls each year.
Data sources
The data for the study were collected from the NSR. A diagnosis of stroke is based on clinical (neurological symptoms persisting more than 24 hours) and radiological MRI findings according to ICD-10 definitions. In Norway, MRI is the standard follow-up imaging modality in all patients admitted to hospital with stroke suspicion, except in a minor proportion with MRI contraindications. CT is performed in these patients. In the acute setting, a plain CT is performed to rule out haemorrhage before the administration of IVT and CT angiography to identify large vessel occlusions eligible for EVT. In patients presenting in the extended time window of 4.5 to 9 hours from symptom onset, CT perfusion was additionally performed to evaluate eligibility for IVT. For patients with unknown symptom onset, defined as wake-up stroke, acute MRI was performed to evaluate eligibility for IVT. Patients examined only with CT were not excluded in our study.
Data collected from the NSR included patient baseline variables, risk factors for stroke (prior transient ischaemic attack (TIA), prior stroke, prior myocardial infarction, known atrial fibrillation, smoking and history of diabetes), National Institutes of Health Stroke Scale (NIHSS) scores at hospital admission, onset-to-hospital admission times, door-to-needle IVT times and door-to-groin EVT times. We also collected the pre-stroke modified Rankin Scale scores (mRS) prior to, and the scores 3 months after the index stroke. The pre-stroke mRS scores are reported to the NSR and are based on previous medical records. Pre-stroke mRS scores and phone-based 3 months post stroke outcome evaluation were performed by a stroke nurse certified in mRS stroke assessment.
Study procedures
Patient data from the NSR cohort were linked to local EMDC databases using unique social security numbers. The patients with AIS were categorised into two groups: those accurately identified with an MPDS stroke suspicion dispatch and AIS patients incorrectly identified and given an alternate MPDS problem code dispatch by the EMDC. The stroke suspicion was defined by the EMDC when an ambulance was dispatched according to MPDS criteria 28.1–28.6 (19). Accuracy was defined as the suspicion for stroke and the patient had a confirmed stroke according to the NSR.
Data collected from the EMS journals included ambulance dispatch criteria, emergency levels (emergency of acute, urgent or routine priority), presence of FAST or non-FAST stroke symptoms (acute dizziness, unconsciousness, diplopia and ataxia) and EMS time intervals. The data collected on non-FAST stroke symptoms included common clinical presentation forms in posterior circulation stroke, where both FAST and NIHSS are inadequate screening tools.17 The EMS interval times collected were dispatch times (time from EMDC contact to ambulance dispatch), response times (time from EMDC contact to ambulance on-scene arrival), EMS on-scene times (time from arrival of the ambulance to departure to hospital) and EMS total prehospital times (time from EMDC contact to hospital admission).
Study outcomes
The primary outcomes of the study were the ambulance on-scene times and the door-to-needle times for IVT eligible patients. The secondary outcomes included the IVT rates, door-to-groin EVT times for eligible patients, proportion of patients with FAST symptoms and the proportion of patients achieving functional independence, as defined by an mRS score of 0–2 3 months after the stroke.
Statistical analysis
For descriptive analyses, we presented categorical variables as numbers (percentage) and continuous variables as median (IQR). We performed the Pearson χ2 test on categorical variables and non-parametric Mann-Whitney U-test on the continuous variables. A binary logistic regression was performed for the association of IVT rates with EMDC stroke suspicion adjusted for age, sex, prior TIA, stroke, myocardial infarction, pre-stroke mRS score and smoking. We also performed a multinomial logistic regression for the association of mRS scores and EMDC stroke suspicions adjusted for age, sex, IVT treatment, EVT treatment and hospital admission <4.5 hours from the symptom onset. The four and a half hour cut-off was chosen because this is the accepted standard time limit for IVT in AIS.18 We also performed a post hoc sensitivity analysis adding prehospital FAST symptoms as confounders in the model. P values ≤0.05 were considered statistically significant. All data analyses were performed using IBM SPSS Statistics V.26 (IBM, Armonk, New York, USA).
Patient and public involvement
A patient representative participated in developing the study design. The representative also participated in drafting the patient information letter.
Results
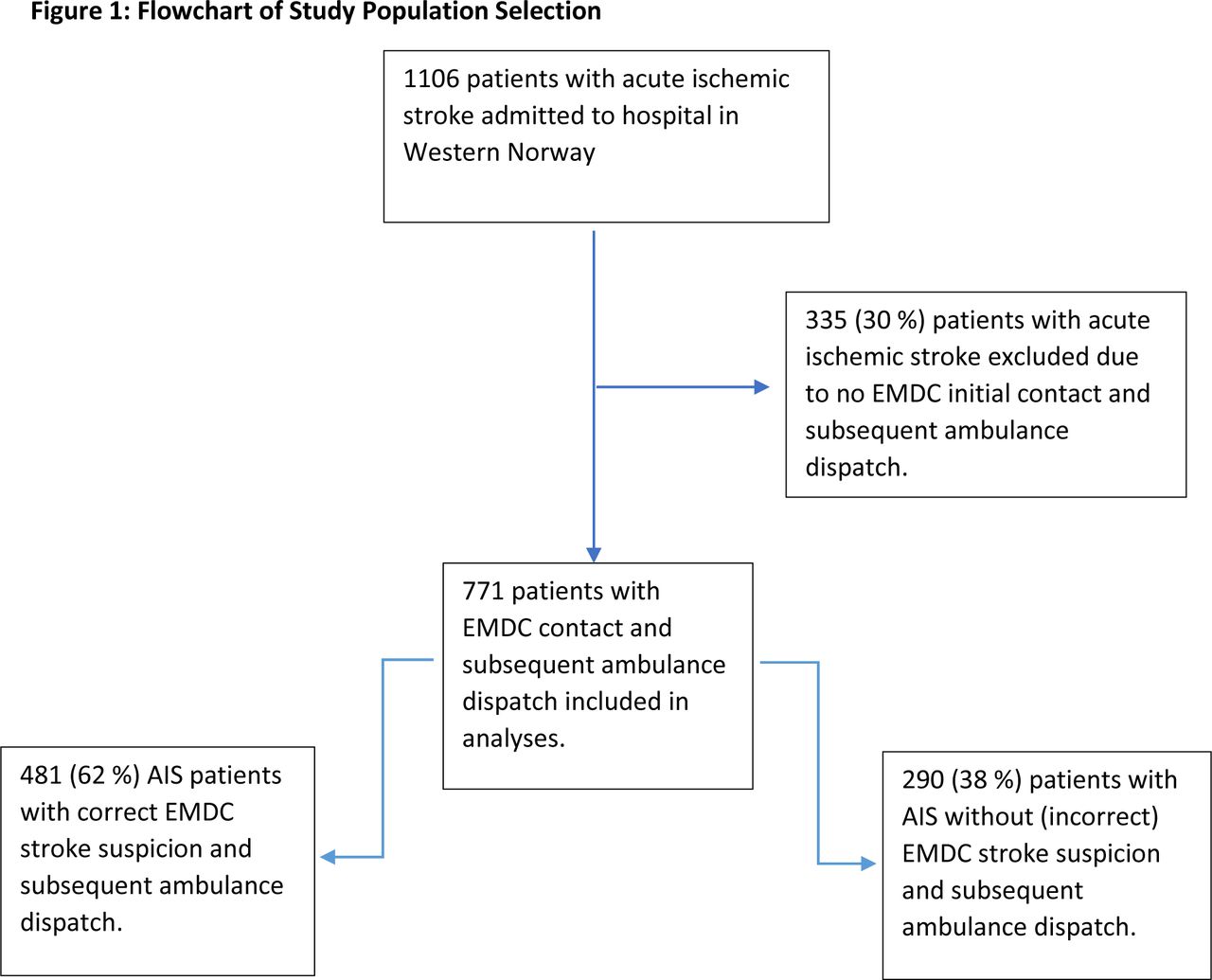
From the NSR, we identified 1106 patients admitted to the hospital with AIS between 1 January and 31 December 2021, from the NSR. Among these, 771 patients (70%) were included based on their initial contact with the EMDC and subsequent transport and admission to the hospital by ambulance.
Baseline characteristics
A flow chart presenting the study population, including the inclusion criteria, categorisation of patients by MPDS stroke suspicion dispatch codes or with MPDS non-stroke suspicion dispatch code, is presented in figure 1. In 481 of the 771 cases (62 %), an ambulance was dispatched with an accurate EMDC suspicion of a stroke.

{kind=link}
Flowchart of study inclusion criteria and the dichotomization of patients with acute ischaemic stroke (AIS) based on Emergency Medical Dispatch Centre (EMDC) stroke suspicion or not. The EMDC performs an assessment of stroke suspicion using the Medical Priority Dispatch System.
Compared to AIS patients without suspicion of stroke, patients with EMDC stroke suspicion were younger (76 vs 78 years; p=0.020), more likely to smoke (20% vs 17 %: p=0.042), less likely to have a history of diabetes (14% vs 24%; p<0.001) and a higher proportion of patients were functionally independent prior to the stroke event (85% mRS 0–2 vs 79% mRS 0–2) (table 1). The NIHSS stroke severity was equal between those with and without stroke suspicion (NIHSS 4 vs 4; p=0.42). No differences were found with regard to prior myocardial infarction, stroke or TIA.
Baseline characteristics of patients with stroke suspicion versus no stroke suspicion at ambulance dispatch
Stroke symptom characteristics
Significant differences in stroke symptoms were observed between the stroke suspicion and non-suspicion group (table 2). Prehospital FAST symptoms recorded by EMS on-scene were more frequent in patients within the EMDC stroke suspicion group (377 (78%) vs 198 (70%); p<0.001). Non-FAST stroke symptoms (acute dizziness, ataxia, unconsciousness, diplopia) were less frequent in this group (101 (21%) vs 87 (30%); p<0.001). Data regarding non-FAST stroke symptoms were missing for three patients (<1%) in the EMDC stroke suspicion group, and for five patients (2%) in the EMDC no-stroke suspicion group.
Stroke symptom characteristics
Primary and secondary outcomes
Patients with an accurate EMDC stroke suspicion experienced more frequent ambulance dispatches with acute priority (462 (96 %) vs 196 (68 %); p<0.001).Both median EMS ambulance on-scene time (11 min vs 15 min; p<0.001) and door-to-needle time (23 min vs 31 min; p=0.023) were shorter in the EMDC stroke suspicion group (table 3). The median EMS total prehospital time (40 min vs 49 min; p<0.001) and door-to-groin time for patients initially admitted to an EVT centre (65 min vs 85 min; p=0.001) were also lower in this group.
Response times, reperfusion treatments and outcomes by EMDC action
After adjusting for age, sex, prior TIA, stroke, myocardial infarction, pre-stroke mRS score and smoking, the EMDC stroke suspicion was still associated with higher IVT rates (OR 2.42 (95% CI 1.72 to 3.40); table 4). In the sensitivity analysis adding prehospital FAST symptoms as confounder in the model, EMDC stroke suspicion was still associated with higher IVT rates, although with a lower effect estimate (OR 1.89 (95% CI 1.29 to 2.75).
Association of EMDC stroke suspicion with administration of intravenous thrombolysis (binary logistic regression)
The mRS 3 months follow-up data were available for 392 (81 %) patients in the EMDC stroke suspicion group and for 243 (84%) patients in the non-stroke suspicion group. There were no differences in the proportion of patient with functional independence (mRS 0–2) between those with and without an EMDC stroke suspicion (240 (61%) vs 160 (66%); p=0.24), even after adjusting for age, sex, pre-stroke mRS scores, IVT administration, EVT administration and admission <4.5 hours after symptom onset (OR 0.80 (95% CI 0.24 to 2.64) (table 5).
Association of modified Rankin Scale (mRS) score 0–2 with EMDC stroke suspicion (multinomial logistic regression)
Discussion
The main message from this study is that an accurate EMDC stroke suspicion alert during dispatching of the ambulance teams was associated with several favourable outcomes, including reduced ambulance on-scene times, lower EMS prehospital times, higher IVT rates, and lower door-to-needle and door-to-groin puncture times. These advantages highlight the importance of EMDC accurate symptom assessment. They underscore the importance that EMDC operators have the required competencies about the heterogeneity in stroke symptom presentations to quickly identify AIS, thus speeding up the acute stroke chain.
We did not observe differences in the NIHSS severity scores on hospital admission between those with and without a suspicion for stroke.
There is limited research on the knock-on effects of EMDC stroke suspicion dispatch performance on overall patient outcomes. Early prehospital on-scene stroke identification and hospital pre-notification play an important role in reducing time delays and improving IVT rates. A national Danish retrospective cohort study from 2023, including all patients with AIS with an EMDC call within 3 hours from symptom onset, found that the identification of patient strokes by the EMDC was associated with reduced prehospital delays and increasing IVT rates, but no differences in EVT rates.19 Other studies also indicate that on-scene stroke identification and hospital pre-notification of stroke by ambulance personnel additionally can reduce in-hospital time and in-hospital mortality.7 20 However, to our knowledge, no studies have demonstrated that accurate EMDC stroke suspicion alerts after a stroke suspicion can simultaneously reduce the prehospital and in-hospital time metrics.
In our study, the EMDC suspected an AIS in 481 of 771 cases, resulting in a sensitivity of 62%. Previous studies from the Western Norway Health Region and Copenhagen Region, Denmark, have found sensitivity rates of 58% and 64%, respectively, for AIS, TIA and intracerebral haemorrhages.21 22 The sensitivity rate in our study aligns with these two studies. Patients with non-FAST stroke symptoms, such as acute dizziness, ataxia, diplopia and unconsciousness, were less likely to receive an EMDC stroke suspicion ambulance dispatch. A Finnish EMDC study from 2019 also found similar results, except for vertigo and ataxia.23 These two symptoms were not associated with higher rates of dispatches with no stroke suspicion.23
A recently published Norwegian study shows that strokes missed by the EMDC were identified by on-scene ambulance personnel in the majority of cases.24 In this study, 94% of strokes were identified either by EMDC or by ambulance personnel on-scene. The authors also found that lack of EMDC identification of stroke was associated with increased hospital delays, which is supported by our finding. Since our system of care and EMS are very similar to this study, we may postulate that a similar proportion of patients are identified in the prehospital setting.
The proportion of patients achieving functional independence (mRS score 0–2) 90 days post-stroke between the two groups was not found to be different in our study, despite significant differences in most prehospital and in-hospital parameters. This differs from prior studies showing that the time from the symptom onset to reperfusion has been proven to be associated with improved stroke outcomes.3 25 Severity of strokes, as determined by NIHSS scores, was not different. The absence of data on the location and volume of the brain infarctions limits our ability to explain the reason for the lack of outcome differences between the groups. Additionally, the mRS primarily focuses on motor function, but patients may also experience other types of health issues. This is particularly relevant for patients with mild strokes who often achieve an mRS score of 0–1 indicating no significant disability, while still having significant deficits in non-motor domains and overall function.26 This may all have influenced why we did not find any differences in mRS post-stroke outcomes.
Our collected data on non-FAST stroke symptoms represent common clinical presentations in patients with posterior circulation strokes, where FAST and NIHSS are inadequate.17 This poses a diagnostic challenge both for EMDC operators, ambulance personnel and stroke physicians. Increasing knowledge of posterior stroke symptom may improve EMDC stroke identification rates. This may lead to more accurate and timely dispatch decisions.27 Most EMDCs in Norway use the MPDS algorithm, which primarily relies on FAST screening. However, evidence suggests MPDS is insufficient.12 There is no consensus on which reference tool is the best for medical dispatch. A meta-analysis from 2018 reviewing the accuracy of medical dispatch found low overall evidence for dispatch accuracy.28 Regarding the reference tools for stroke identification, the authors concluded that it was not possible to suggest a superior-based dispatch system.28
The study underscores the crucial role of EMDCs in early stroke identification. An Utstein template for emergency stroke care has been developed, emphasising the five important factors for improved patient outcomes: bystander identification, early recognition, dispatch by the EMDC, prehospital on-scene stroke assessment, rapid initiation of reperfusion treatment and early rehabilitation and follow-up.29
Our study has several limitations. First, as a retrospective registry-based observational study, the study has an inferior level of evidence compared with prospective studies and does not allow us to establish causal relationships. Second, the study was conducted in a specific region of Norway, potentially limiting generalisability to other settings and countries which have very different EMS and public health systems, finances and emergency medical services coverage. Third, we only included patients diagnosed with AIS (ICD-10 I63) and did not collect patient data on false-positive MPDS stroke suspicion dispatches communicated to ambulances. Specificity in EMDC stroke dispatch could not therefore be evaluated. Fourth, there may be confounding factors that cannot be controlled for and were not considered in the analysis to the extent that clinical trials can. Finally, the variability in the quality and type of the collected data, absence of data pertaining to long-term and functional outcomes, prehospital information, and complications as well as other methodological obstacles limits the utility of registry data in clinical and epidemiological research. One example is that we collected limited data on visual symptoms such as diplopia. A systematic review from 2023 provides evidence that acute visual impairment is present in a significant proportion of patients with strokes and visual impairment may present in a heterogeneous way.30
Conclusions
This study found that accurate stroke suspicion by the EMDC is associated with a reduction in time delays to treatment and can increase the proportion of patients eligible for early stroke reperfusion treatments. Enhancing the EMDC’s sensitivity in suspecting strokes during dispatch may improve the overall acute stroke chain care for patients with AIS and also impact long-term patient outcomes. Future research is needed on strategies to improve the accuracy of stroke detection during the EMDC dispatch and potentially enhancing the overall effectiveness of the stroke care systems and improving patient stroke outcomes.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Western Norway Regional Health Ethics Committee (ID461919). The study was approved by the Western Norway Regional Health Ethics Committee in 2022 (ID461919). Informed consent was not obtained, but all patients received an information letter describing their ability to withdraw from the study at any time without impacting their care.
Acknowledgments
We would like to thank the Norwegian Stroke Registry and local EMS services for sharing data for the conduction of this study. We would also like to thank the donor from the Maria Mirjam Katerina Sula Evjen trust to enable the completion of this study.
References
Footnotes
Handling editor Ellen J Weber
Contributors NL contributed to conceptualization, data collection, formal analysis, original draft preparation, editing and revision. LH and HL contributed to data collection, validation, drafting, editing and revision of the manuscript. MB, HL, AF, MK, ØØ, CB and LH contributed to validation, drafting, editing and revision of the manuscript. EF, PB and TL contributed to conceptualization, validation, drafting, revision and editing of the manuscript. NL is fully responsible for the conduct of the study, had access to the data and controlled the decision to publish. NL is the guarantor for this study and takes full responsibility for the work, conduct of study, had access to the data, and controlled the decision to publish.
Funding The completion of the study and presentation of findings at scientific congresses was financed by grants from the Maria Mirjam Katerina Sula Evjen trust, Inger Valsøes foundation for neurological research and the Norwegian foundation for anaesthesia research. The grant providers had no influence on the final published article.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.